Case 8: Multiple sclerosis
A 38-year-old woman presented with tingling, numbness and
clumsiness of both hands for 1 week, with a band of numbness from the umbilicus
to the axillae. Six months earlier, following an upper respiratory tract
infection, she had experienced paraesthiae in the feet, numbness from the waist
downwards and 'burning' pains behind the right ear. She was anxious because her
maternal grandmother had suffered from multiple sclerosis. On neurological
examination, she had absent abdominal reflexes with brisk tendon jerks and
bilateral extensor plantar responses. Blood results were normal: Haemoglobin, white-cell count
and differential, erythrocyte sedimentation rate, vitamin B12 and folate levels
and syphilis serology. The cerebrospinal fluid (CSF): Protein concentration
0.4g/l (NR 0-0.4g/l) , –Red blood cells:None, Lymphocytes 3 x 106/l (NR <5 x
106/l), IgG concentration 123mg/l (NR <60mg/l), Albumin concentration
470mg/l (NR <400mg/l), IgG/albumin ratio 26% (NR 4-22%), IgG index 1.07 (NR
<0.7) , Isoelectric focusing Oligoclonal bands present .
Summary
Multiple sclerosis
(MS) is primarily an inflammatory disorder of the brain and spinal cord in
which focal lymphocytic infiltration leads to damage of myelin,
oligodendrocytes and axons. Initially, inflammation is transient and
remyelination occurs but is not permanent. The early course of disease is
characterized by episodes of neurological dysfunction that usually recover.
However, over time the pathological changes become dominated by widespread
microglial activation associated with extensive and chronic neurodegeneration.
Chronic neurodegeneration, which is progressive, leads to accumulation of
sensory and motor disabilities.
Paraclinical
investigations show abnormalities that indicate the distribution of
inflammatory lesions and axonal loss, interference of conduction in previously
myelinated pathways,and intrathecal synthesis of oligoclonal antibody1.
Multiple sclerosis is
triggered by environmental factors in individuals with complex genetic-risk
profiles. Before 1980 it was found a greater incidence of MS in higher
latitudes. However, later it was demonstrated also a high prevalence in lower
latitudes, a fact that reveals a possible environmental influence2. Other element that indicated
environmental influences are an increased risk of MS among individuals with a
history of mononucleosis, a marker of late infection with the Epstein-Barr
virus, have an increased risk of MS3.
On the other hand,
first-degree relatives had a sevenfold increased risk of developing MS, with an
incidence of 0.5% in women and 0.3% for men. Furthermore, 20 identified loci
have been linked to MS. DRB1 alleles and HLA-A gene variations are implicated
with T helper development, being a determinant factor during MS pathogenesis4.
Determination of
protein biomarkers is being correlated to MS, demonstrating potential
predictors of the disease. Inward rectifying potassium channel KIR4 was
identified as a target of IgG. Interestingly, serum levels of IgG to KIR4 were
higher in patients with MS; leading to less KIR4 expression, altered expression
of glial fibrillary acidic protein in astrocytes, and activation of complement cascade
at the sites of KIR4. Additionally, albumin is not synthesized in central
nervous system; therefore, its presence in cerebral spinal fluid gives
indication of blood brain barrier (BBB) disruption5.
T-helper 17
lymphocytes appear to be essential for inflammatory diseases. It was demonstrated
the expression of IL-17 and IL-22 receptors on BBB endothelial cells (BBB-ECs)
in MS lesions, demonstrating to play a role in the rupture of BBB tight
junctions. Furthermore, T-helper 17 lymphocytes transmigrate efficiently across
BBB-ECs, highly express granzyme B, kill human neurons and promote central
nervous system inflammation through CD4+ lymphocyte recruitment6.
Although there is no
cure for MS, immunosuppresants and steroids are used to treat the disease.
Glatiramer acetate is believed to reduce the malfunction of lymphocytes by
reducing its activation. Oral
administration of Laquinimod induces repair of damaged neuronal tissue,
stimulating the release of brain derived neurotropic factor (BDNF). In
addition, Teriflunomide inhibits the synthesis of pyrimidine, limiting the
proliferation of lymphocytes. In this way, the immune system is suppressed,
decreasing inflammation and myelin degeneration of the central nervous system.
Questions
Question 1: What neurological functions/structures are
affected in the patient?
The patient currently
presented with tingling, numbness, and clumsiness of both hands for 1 week and
with a band of numbness from the umbilicus to the axillae. Sensory symptoms are
common initial feature of MS, which include symptoms such as numbness,
tingling, pins/needles, tightness, coldness, or swelling of limbs or trunk,
which can de due to demyelination or lesion to sensory tracks in the CNS
leading to the cerebral cortex. The patients clumsiness is due motor symptoms
from the lesion of the descending motor tracts of the spinal cord and
cerebellar pathways, which help originate and coordinate movement. The band of
numbness from the umbilicus (thoraxic T10)-axillae (thoraxic T4) can be
explained by a lesion to the spinothalamic tracts in the CNS.
The patient has a
history of paresthesia in the feet, numbness from the waist down, and burning
pains behind here right ear that after an upper respiratory infection, but then
subsided after infection. In patients with MS, this is a sign called Unthoff’s
phenomenon7.Unthoff’s phenomenon is due to an
increase in temperature that temporarily worsens neurological symptoms in MS
patients due to the effect of temperature on nerve conduction, an increase in
temperature can impulse, slow or block nerve conduction. Once temperature
decreases (after infection), the symptoms decrease or subside.
Upon neurological
exam the patient had absent abdominal reflexes, which means she lost her
superficial reflexes due to an upper motor neuron lesion. In addition, she
showed to have a positive Babinski sign by bilateral extensor plantar
responses, which are also a sign of an upper motor neuron lesion. These upper
motor neuron lesions can be due to demyelination or lesion of a part of the
corticospinal tracks that begin at the cerebral cortex and terminate at the
ventral horns of the spinal cord.
Question 2: What type of immunological mechanisms can
explain the alterations observed in the patient?
Inflammation,
demyelination and axon degeneration are the major causes of the alterations
observed in this patient and are commonly seen in patients with MS1.
Initially, an unknown inflammation at the brain alters the blood brain
barrier and disrupts the tight junctions, which allows leukocytes to enter.
T-cells specific for CNS antigen activate complement, activate macrophages
(microglia), and recruit more leukocytes. The T-cells are specific for myelin
protein antigen, and oligodendrite antigens8. This t-cell medicated activation
caused the tissue damage and demyelination of CNS axons, which led to motor and
sensory deficits seen in the patient.
Risk Factors
There are a series of
risk factors that make development of MS more probable. For example relatives
of a person with the disease are at a higher risk than the general population.
Differences in the human leukocyte antigen (HLA) system—a group of genes in
chromosome that serves as the major histocompatibility complex (MHC) in humans—
specifically DR15 and DQ6, increase the probability of suffering MS. On the
other hand it is interesting to note that other loci such as HLA-C554 and HLA-DRb11
have shown a protective effect. Meaning that presence of these alleles actually
reduces probability of contracting the disease.
Some viral infections
have also been associated with development of MS. Human herpes viruses are a
candidate group of viruses linked to MS. Also individuals infected with
Epstein-Barr virus as young adults have a greater risk of developing the
disease. Because of this there’s a higher incidence of the disease in places
where these viruses are more common.
Below is a list of the
most common risk factors for MS:
Virus
|
A viral infection can be a risk
factor for MS.
|
Age
|
Multiple Sclerosis is more common in persons between 15 –
40.
|
Gender
|
Women have a higher risk of suffering MS.
|
Family History
|
There is a genetic factor involved in the risk of MS.
|
Weather
|
Multiple Sclerosis is more common in persons who live in
cold weather.
|
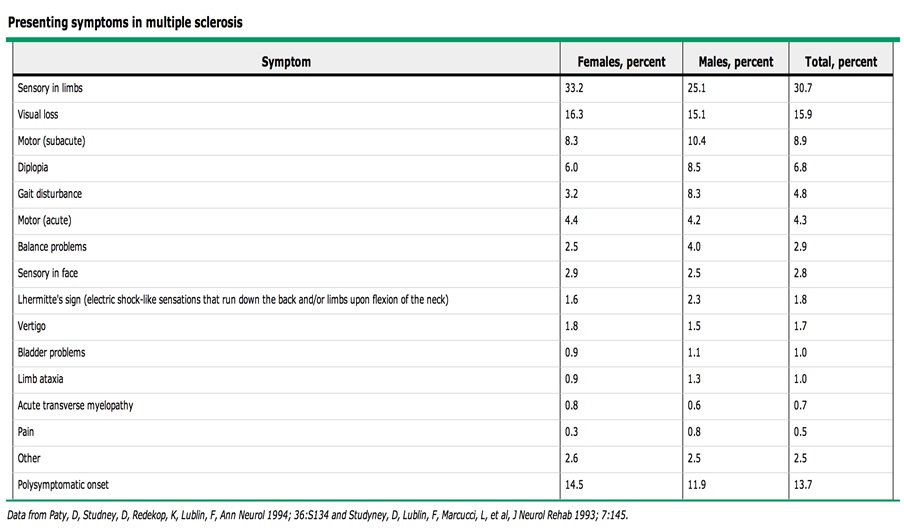
Symptoms
Below is a list of
the most common presenting symptoms in MS:
Clinical Correlations
Achieving an ultimate
multiple sclerosis (MS) diagnosis is not always simple. Many neurological
conditions may mimic MS symptoms and make diagnoses confusing. Vitamin B12
deficiency for example, is an absence in vitamin B12 which can cause myelin
damage, including a myelopathy, and thus mimic MS. Neuropathies involving
the dorsal columns and the corticospinal tract may also mimic MS symptoms. For
these reasons diagnosis of MS should be done through a careful collection of
historical, genetic, evoked potentials, neuroimaging and laboratory information9.
MS is the result of
an initial atypical inflammation on the central nervous system leading to
T-cell CD4+ activation by microglial cells. Activation of T-cell CD4+ cells
further increases attack on antimyelin antibodies for myelin oligodendrocyte
glycoprotein MOG and myelin basic protein MBP are potential markers of MS
activity and predictors of progression of MS10. Inflammation and damage to these
tissues leads to the characteristic lesions (scleroses) seen in scans of MS
patients. MRI tests are the gold standard in diagnosing MS, due to higher
sensitivity for these lesions11. Other tests to diagnose multiple
sclerosis include a lumbar puncture to look for the presence of proteins,
leukocytes, immunoglobulins. The presence of albumin in cerebral spinal fluid
implies disruption of the blood brain barrier indicating inflammation. An
abnormality of CSF IgG production is measured by the IgG index. IgG and albumin
ration is next calculated and is an indicator of a positive test for MS12. The presence of oligoclonal bands is
common in 95% of patients with MS13. Oligoclonal bands are the result of
chronic central nervous system infections, viral syndromes, and neuropathies.
Figures





References
1. Compston A, Coles A. Multiple sclerosis. Lancet.
2008;372(9648):1502–17. doi:10.1016/S0140-6736(08)61620-7.
2.
Alonso A, Hernán M a. Temporal trends in the incidence of multiple sclerosis: a
systematic review. Neurology. 2008;71(2):129–35.
doi:10.1212/01.wnl.0000316802.35974.34.
3.
Hernan MA, Zhang SM LL. Multiple sclerosis and age at infection with common
viruses. Epidemiology. 2001;12.
4.
Nielsen NM, Westergaard T, Rostgaard K et al. Familial risk of multiple
sclerosis: a nationwide cohort study. Am J Epidemiol. 2005.
5.
Srivastava R, Aslam M, Kalluri SR, et al. Potassium channel KIR4.1 as an immune
target in multiple sclerosis. The New England journal of medicine.
2012;367(2):115–23. doi:10.1056/NEJMoa1110740.
6.
Kebir H, Kreymborg K, Ifergan I et al. Human TH17 lymphocytes promote
blood-brain barrier disruption and central nervous system inflammation. Nat
Med. 2007.
7.
Uhthoff_and_His_Symptom.2.pdf.
8.
Zhang BJ, Markovic-plese S, Lacet B, Raus J, Weiner HL, Hailer DA. From the
*Center for Neurologic Diseases, Division of Neurology, Department of Medicine,
Brigham and Women’s Hospital and Harvard Medical School, Boston, Massachusetts
02115; and the *Multiple Sclerosis Research Laboratory, Dr. L.
Willems-Instituut, Universitaire Campus, B-3590 Diepenbeek, Belgium.
1994;179(March).
9.
Poser CM, Paty DW, Scheinberg L, et al. New diagnostic criteria for multiple
sclerosis: guidelines for research protocols. Annals of neurology.
1983;13(3):227–31. doi:10.1002/ana.410130302.
10.
Berger T, Rubner P, Schautzer F, et al. Antimyelin antibodies as a predictor of
clinically definite multiple sclerosis after a first demyelinating event. The
New England journal of medicine. 2003;349(2):139–45.
doi:10.1056/NEJMoa022328.
11.
Filippi M, Rocca MA. MR Imaging of Multiple Sclerosis 1 n STATE OF THE ART.
2011;259(3):659–681.
12.
McLean BN, Luxton RW, Thompson EJ. A study of immunoglobulin G in the
cerebrospinal fluid of 1007 patients with suspected neurological disease using
isoelectric focusing and the Log IgG-Index. A comparison and diagnostic
applications. Brain : a journal of neurology. 1990;113 ( Pt 5:1269–89.
Available at: http://www.ncbi.nlm.nih.gov/pubmed/2245296. Accessed May 10,
2013.
13.
Statement AC. Recommended Standard of Cerebrospinal Fluid Analysis in the
Diagnosis of Multiple Sclerosis. 2005;62(June).
La Universidad de Adelaide en el sur de Australia anuncio recientemente que tiene esperanzas de utilizar celulas madres de tejido adiposo, para enviar celulas con propiedades anti-inflamatoria al lugar de la lesion en el CNS para tratar MS. Los investigadores anunciaron que el problema es dirigir o insertar estas celulas en el lugar de la lesion ya que cuando se inyectan en el torrente sanguineo bien pocas cruzan el BBB. Los investigadores esperan que con ciertas modificaciones que le hagan a estas ellas puedan cruzar el BBB con mas facilidad.
ResponderBorrarhttp://www.heraldsun.com.au/news/university-of-adelaide-research-raises-hope-for-multiple-sclerosis-treatment/story-e6frf7jo-1226639700275
Other than the above mentioned symptoms, a patient may present with different cognitive symptoms that are more prevalent in the areas of memory and processing speed. Lesions of the CNS associated with these processes are common. Also, a current topic in the literature is the possible relationship between Vitamin D deficiency and MS progress. In Puerto Rico there is an unusually high incidence of Vitamin D deficient patients. For this reason a Puerto Rican patient with MS can benefit from taking supplements with high vitamin D content.
ResponderBorrarlol, let them know H!
BorrarEste comentario ha sido eliminado por el autor.
ResponderBorrarAunque no precisamente en este caso, es importante destacar que además de los síntomas y daños motores y sensoriales que se mencionan aquí, los pacientes de esclerosis múltiple también presentan depresión. Es posible pensar que estas personas expresan cierto grado de tristeza y cambios de ánimo debido a la difícil situación que enfrentan, pero la realidad es que además de la tristeza normal que puede presentar una persona que está consciente de su enfermedad, estos pacientes sufren depresión. Esto se debe principalmente a que a medida que progresan las lesiones se afectan otras estructuras en el cerebro, particularmente, el sistema límbico.
ResponderBorrarSe considera que la mitad de los pacientes de esclerosis múltiple sufren depresión, esto a su vez los expone a un mayor riesgo de suicidio comparado con la población general. Además de los síntomas evidentes de la depresión, se puede utilizar los MRI’s que se le practican a estos pacientes para ver el grado del daño al sistema límbico.
This is a very good collection of information, but i feel like the psychological symptoms were ignored. Cognitive impairments and depression are just as important as double vision. As future doctors we need to stop neglecting the psychology and start thinking about every aspect of a disorder. Socio-Biomedical model is here to stay and will define the future of medicine. Thank you!
ResponderBorrarI agree with you buddy....MY MAN!
BorrarMS is a life changing disease in which once the patient is diagnose, treatment should start immediately so the condition can be control and delayed as much as possible. Nowadays there are a great number of drugs that can help diminish this patients relapses. Among all the drugs available to treat MS, natalizumab or better known by its brand name tysabri, its particularly interesting to me. Tysabri is a monoclonal antibody against alpha 4 integrin. This drugs helps in keeping white blood cells from getting into the brain and attacking nerves. Tysabri has shown to improve three aspects of MS: it reduces flare ups, slows down the progression of physical disabilty and reduces new brain lesions. What is particularly interesting to me is that it was found that this drug increases the risk of progressive multifocal leukoencephalopathy (PML), which is a rare disease of the brain cause by the JC virus. PML usually causes death or great disability. Usually the risk for MS patients increase after two years of using tysabri. It is amazing how this and other drugs can help in different health conditions but at the same time have such potential side effects.
ResponderBorrarIt's interesting that MS is only found in Northern Hemispheres, particurly more in females. Do you think it has to do with the amount of sun light those in the northeast don't recieve? Or could it possibly be due to more air pollutants in a congested environment
ResponderBorrarYes Michael, current research is looking at the possible levels of sun exposure and vitamin D concentrations. A few studies are actually being done now, but data hasn't been consistent enough to make the conclusion that vitamin d levels as a risk factor for MS.
ResponderBorrar